- Visibility 132 Views
- Downloads 32 Downloads
- DOI 10.18231/j.jeths.2024.014
-
CrossMark

Cooperative dynamics in surgical training: Applying Axelrod's game theory principles to enhance surgery education
- Author Details:
-
 Zayapragassarazan Z
Zayapragassarazan Z
-
Devi Prasad Mohapatra *
Introduction
The landscape of medical education, particularly in the territory of surgical training, presents a complex interplay of challenges that demand innovative solutions. At the heart of these challenges lies the need to ensure that trainee residents not only acquire the requisite technical skills and knowledge but also develop the professional demeanor and decision-making abilities critical to patient care and surgical excellence. The dual necessity of maximizing educational outcomes while maintaining the highest standards of patient safety underscores the need for an educational paradigm that effectively balances these priorities. Yet, traditional models of surgical training, often characterized by hierarchical structures and varying degrees of mentorship, sometimes fall short in fostering an environment conducive to optimal learning and professional development. [1], [2]
The concept of game theory, a mathematical framework that explores strategic interactions among rational decision-makers, can be applied in this environment.[3], [4] Originating in economics to analyze competitive situations where the outcome for each participant depends on the actions of all, game theory has since transcended disciplinary boundaries, offering valuable insights into the dynamics of cooperation and conflict across a range of human endeavors.[5] In the context of medical education, game theory provides a novel lens through which to examine the intricate dynamics between educators and learners. Specifically, the Iterated Prisoner's Dilemma, a cornerstone of game theory explored by Robert Axelrod, offers a rich theoretical foundation for understanding how cooperative behaviors can emerge and be sustained even in competitive environments.[6]
The objective of applying Axelrod's game theory to surgery training is twofold. First, it aims to conceptualize the educator-learner relationship in surgical training as a series of strategic interactions, providing a structured framework to navigate the complexities of this relationship. Second, by leveraging the principles derived from the Iterated Prisoner's Dilemma—such as reciprocity, trust, and the long-term benefits of cooperation—this approach seeks to enhance the efficacy of surgical training programs.[7], [8], [9] In doing so, it promises not only to improve educational outcomes for residents but also to contribute to a culture of excellence and collaboration in the surgical profession. This manuscript aims to outline a theoretical framework that applies game theory to the specific context of surgical training, with the ultimate goal of fostering a more cooperative, dynamic, and effective learning environment.[10], [11]
Overview of game theory, prisoner’s dilemma and the iterated prisoner's dilemma
At its core, game theory seeks to understand how individuals can optimize their outcomes in situations where success is interdependently linked, revealing the intricate balance between conflict and cooperation. Through its fundamental concepts and models, such as the Nash Equilibrium and the Prisoner's Dilemma, game theory provides a powerful framework for analyzing decision-making processes in competitive environments. The concept of the Prisoner’s Dilemma illustrates how two rational agents might not cooperate, even when it is in their best interest to do so. The Iterated Prisoner's Dilemma (IPD), an extension of this basic dilemma, involves repeated interactions between the same participants, allowing for the evolution of strategies over time. The IPD is particularly relevant to understanding complex social behaviors, as it demonstrates how cooperation can emerge through reciprocity and trust, despite the temptation to defect for immediate gain.
Prisoner’s Dilemma is a classic game theory scenario that exemplifies the tension between individual and collective benefit. In this scenario, two individuals, unable to communicate, must choose between cooperating or defecting. While defecting offers a short-term advantage, mutual cooperation leads to a better outcome for both parties. However, the dilemma arises because the optimal choice for each individual, assuming the other will defect, is also to defect. This creates a situation where both individuals end up worse off than if they had cooperated.
Axelrod's Iterated Prisoner's Dilemma builds upon this concept by introducing the element of repeated interactions. Players encounter each other multiple times, allowing them to adapt their strategies based on their opponent's past actions. Through a series of tournaments, Axelrod explored which strategies would lead to optimal outcomes in this iterated setting. He discovered that Tit-for-Tat (TFT), a strategy that cooperates initially and then mirrors the opponent's subsequent actions (cooperate for cooperation, defect for defection), emerged as the most successful approach. TFT promotes cooperation by establishing trust and encouraging continued collaboration while also deterring defection through measured retaliation. This finding holds significant implications for understanding cooperation in various contexts, including the dynamic relationship between educators and learners in surgical training.
Summary of Axelrod's findings and principles
Robert Axelrod's exploration of the IPD through computational tournaments revealed surprising insights into the nature of cooperation. The strategy of "Tit for Tat," which involves starting with cooperation and then mirroring the opponent's previous move, emerged as a robust approach to achieving mutual cooperation. Axelrod distilled the success of "Tit for Tat" into four key principles: niceness (never being the first to defect), retaliation (responding to defection with defection), forgiveness (returning to cooperation if the opponent does), and clarity (being predictable and understandable to others). These principles underscore the importance of a balanced approach to competition and cooperation, highlighting the potential for stable, mutually beneficial outcomes even in adversarial settings.
The conceptual framework
In a busy university hospital, ‘M’, a renowned plastic surgeon known for her meticulous techniques and dedication to teaching, was preparing her team for a complex surgery to correct a patient's claw hand, a condition often resulting from ulnar nerve injury. Among her team is ‘L’, a keen but sometimes overwhelmed surgical resident, eager to learn but struggling to balance the demands of his training.
One day, prior to the scheduled surgery, M called upon L.
M: "Tomorrow's surgery is not just about correcting a deformity. It's about restoring function and hope. I need you to thoroughly understand the anatomy and pathology of ulnar nerve injury. Please, make sure you read up on it tonight. It will be crucial for your learning and our patient's care."
L: "Of course, Dr. M. I'll make it a priority,"
However, Emergency cases, and unexpected consultations, left L unable to complete the assigned task.
The next morning in the operating theatre, M turned to L, expecting a discussion on the ulnar nerve's intricacies. L admitted, "I'm sorry, Dr. M didn't manage to read up last night."
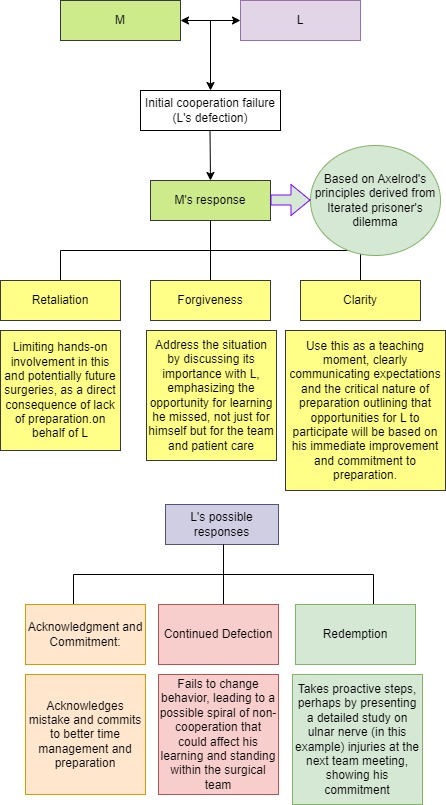
M was disappointed. Yet, the surgery proceeded, with M taking extra time to explain each step and its significance to the anatomy L had failed to review, ensuring the patient's care remained paramount.
This anecdote demonstrates a scenario not uncommon in many surgical residencies. An analysis of the scenario and responses ([Figure 1]) will help in understanding the importance of cooperation, the potential for conflict resolution, and the critical role of clear communication in the mentor-learner dynamic within the high-stakes environment of surgical training.reconceptualizing these interactions as strategic games where decisions to cooperate or defect can lead to different educational outcomes, this framework aims to identify strategies that promote a more collaborative, effective, and mutually beneficial training environment. The essence of this approach lies in fostering an atmosphere where cooperative behaviors are encouraged and rewarded, aligning the interests of teachers and residents towards common goals of learning, professional growth, and patient care.
In the context of this game-theoretical framework, the teacher ('M') and the resident ('L') are considered as players in an iterated game, where each interaction represents an opportunity to either cooperate (such as engaging in constructive teaching and learning activities) or defect (such as withholding information or effort). 'M' embodies the role of mentor, educator, and evaluator, whose actions significantly impact the learning environment and the resident's professional development. Conversely, 'L' represents the learner, whose engagement, effort, and responsiveness to feedback are critical to the educational process. The decisions made by 'M' and 'L' in various situations are influenced by past interactions, anticipated future encounters, and the overall goals of the surgical training program.
Cooperation and defection scenarios in surgical training
Cooperation in this framework is defined as any action by 'M' or 'L' that contributes positively to the learning experience and professional development of the resident or the teaching objectives of the teacher. Examples include 'M' providing personalized feedback and learning opportunities based on 'L''s needs, and 'L' actively engaging in learning activities and applying feedback to improve. Defection, on the other hand, refers to actions that undermine these objectives, such as 'M' neglecting educational duties in favor of other responsibilities, or 'L' not taking full advantage of the learning opportunities provided.
The framework suggests several scenarios illustrating the outcomes of cooperative and defection behaviors:
Mutual cooperation: Both 'M' and 'L' engage fully in the educational process, leading to optimal learning outcomes, professional growth for 'L', and teaching satisfaction for 'M'.
One-sided cooperation/defection: One party consistently cooperates while the other defects, resulting in frustration and suboptimal outcomes for the cooperative party, potentially diminishing overall educational effectiveness.
Mutual defection: Both parties disengage from their educational roles, leading to a deteriorating learning environment and minimal professional development.
This game-theoretical approach to surgical training emphasizes the importance of strategies that encourage cooperation, recognizing that the most beneficial outcomes arise from sustained collaborative efforts.
Discussion
Applying game theory principles to surgical training can significantly enhance cooperation between teachers and residents.[5], [6] In addition to enhancing learning outcomes, this cooperative dynamic is expected to foster professional growth of the mentor (through a sense of from the fulfillment of successfully mentoring the next generation of surgeons) and learners (through accelerated skill development and a development of a stronger professional identity) and inculcate a culture of continuous improvement (through a process of ongoing evaluation and refinement of teaching and learning strategies).[7], [8]
Application of Axelrod's principles
Applying Axelrod's principles of niceness, retaliation, forgiveness, and clarity to surgical training is expected to foster a more positive, productive, and cooperative learning environment.
Niceness: Initiating Cooperation; in the context of surgical training, translates to initiating interactions with a presumption of cooperation. For the teacher ('M'), this might involve proactively offering support, resources, and encouragement to residents ('L'), creating a learning environment that values openness and mutual respect. For residents, being nice could manifest as taking initiative in their learning, showing enthusiasm, and respecting the time and efforts of their teachers and peers. An example of implementing niceness could be 'M' setting aside extra time to discuss cases with 'L', even outside of regular hours, fostering a culture of dedication and mutual respect.
Retaliation: Addressing Non-Cooperation: though a seemingly negative term, is about responding appropriately to non-cooperative behaviors to maintain the integrity of the educational environment. This does not mean punitive measures but rather structured responses that encourage a return to cooperative behavior. For instance, if 'L' repeatedly shows disinterest or neglects responsibilities, 'M' might respond by temporarily increasing supervision or requiring 'L' to reflect on their actions through additional assignments. Conversely, if 'M' is perceived as not providing adequate support, 'L' could express concerns through formal feedback channels, prompting a constructive dialogue.
Forgiveness: Re-establishing cooperation; is crucial for moving past conflicts or periods of non-cooperation. It involves giving the other party the opportunity to return to cooperative behaviors without holding past actions against them. An example might be 'M' recognizing efforts by 'L' to improve after a period of neglect, thereby resuming normal support and mentorship levels. Similarly, 'L' might acknowledge and appreciate improvements in 'M''s engagement or teaching methods, reinforcing positive changes.
Clarity: Promoting Understanding and Predictability; involves ensuring that intentions, expectations, and feedback are communicated transparently and effectively. In surgical training, this could mean 'M' providing clear, actionable feedback on 'L''s performance, along with explicit guidance on how to improve. It also entails 'L' being open about their learning needs and challenges. Implementing clarity might involve structured feedback sessions, clear documentation of goals and outcomes, and regular check-ins to adjust expectations as needed.
Assumptions and noises
For the application of Axelrod's principles from the Iterated Prisoner's Dilemma to work effectively in the training environment between plastic surgery teachers ('M') and residents ('L'), certain assumptions must be in place. However, the possibility of potential "noises" or disturbances that could impact the successful practice of this theory should be kept in mind.
Assumptions for the system to work
Rationality of participants: Both 'M' and 'L' are assumed to be rational actors who understand the benefits of mutual cooperation and are motivated by a desire for optimal outcomes in training and professional development.
Repeated interactions: The theory assumes that 'M' and 'L' will have multiple interactions over time, allowing for the development of trust and the opportunity for retaliatory or forgiving actions to have their intended effect.
Clear communication: Effective and clear communication is assumed, so that intentions and actions are correctly understood by all parties.
Awareness of consequences: Both 'M' and 'L' are aware of the consequences of their actions, including the benefits of cooperation and the costs of defection.
Ability to identify and correct mistakes: A system for feedback and improvement is in place, allowing both 'M' and 'L' to recognize and correct their mistakes.
Possible Noises in the Training Environment
Miscommunication: Misunderstandings between 'M' and 'L' about expectations, feedback, or actions can lead to perceived defections, even when none were intended.
Mismatched goals or values: If 'M' and 'L' have fundamentally different goals or values, it may be difficult to find a basis for cooperation.
External pressures: Stress, workload, external evaluations, and personal issues can affect the behavior of 'M' and 'L', leading to actions that might be misinterpreted as defections.
Limited resources: Constraints on time, attention, or educational resources can lead to competition rather than cooperation, undermining the principles of the Iterated Prisoner's Dilemma.
Fluctuating commitment: Fluctuations in 'M' or 'L''s commitment to the training process, possibly due to external influences or changing personal circumstances, can disrupt the cycle of cooperation.
Perception of inequity: If either 'M' or 'L' perceives the relationship or outcomes as inequitable, it may lead to defection as a form of protest or compensation.
To mitigate these noises and ensure the system works as intended, it's essential to foster an environment that promotes understanding, addresses miscommunications promptly, aligns goals and values, manages external pressures effectively, ensures equitable access to resources, and maintains commitment to the educational process. Regular feedback sessions, open lines of communication, and mechanisms for resolving conflicts can help in navigating these challenges and sustaining a productive and cooperative training environment.
Implications for surgical training
The application of game theory to surgical training presents a unique opportunity to reframe the educational challenges and dynamics between teachers and residents. This theoretical approach offers potential benefits in the form of improved educational strategies, enhanced conflict resolution optimized decision-making.
Future Directions
The proposed conceptual framework, grounded in game theory and specifically Axelrod's principles, presents a novel approach to enhancing surgical training. To validate and refine this framework, several empirical research directions are suggested. Firstly, controlled experiments within surgical training programs could be designed to test the effectiveness of game theory-based interventions on cooperation, learning outcomes, and professional development. This could involve comparing traditional training groups with those where Axelrod's principles are explicitly applied and communicated. Secondly, longitudinal studies could assess the long-term impacts of game theory-inspired strategies on the careers of surgical residents, including their technical proficiency, professional growth, and collaboration within healthcare teams. Thirdly, qualitative research methods, such as interviews and focus groups, could be employed to explore the perceptions of teachers and residents regarding the implementation of game theory principles in their training, providing insights into practical challenges and opportunities. Finally, cross-institutional comparisons could be made to identify best practices and contextual factors influencing the effectiveness of these strategies by comparing surgical training outcomes across institutions with varying degrees of adherence to game theory principles.
Furthermore, this conceptual framework with principles rooted in game theory has the potential for broad application in other fields apart from surgical training. While this manuscript looks specifically into game theory application in surgical training, broad applications in medical education can be identified. ([Table 1]) The emphasis on cooperation, conflict resolution, and continuous improvement is relevant across the spectrum of medical education, making it worthwhile to explore the applicability of game theory principles in other medical specialties, nursing education, and interdisciplinary healthcare team training. Additionally, the game theory framework could be applied to foster cooperation and improve outcomes in interprofessional healthcare teams, thereby enhancing the quality of patient care by optimizing teamwork among healthcare professionals with diverse expertise.[12], [13] Moreover, investigating the use of game theory to inform healthcare policy and administration, particularly in areas related to resource allocation, healthcare delivery models, and patient engagement strategies, could contribute to more effective and equitable healthcare systems by leveraging the principles of cooperation and strategic decision-making.[14], [15]
|
Application |
Description |
|
Promoting Cooperative Learning |
Understanding game theory helps educators create a friendly learning environment where students work together on group projects, boosting their motivation and success. |
|
Teaching Social Skills |
Game theory informs educators on creating learning situations for teaching students’ important social skills like teamwork and negotiation, preparing them for real-life situations. |
|
Using Rewards and Incentives |
Game theory informs about the use of rewards and incentives to encourage good behaviour and active participation among students. |
|
Enhancing Peer Feedback |
In any educational training, feedback from peers helps students learn from their mistakes and become better collaborators and problem-solvers. An understanding of game theory will enhance the quality of feedback. |
|
Effective Classroom Management |
Game theory guides teachers in managing classrooms effectively, promoting cooperation and fairness among students. |
Conclusion
Applying game theory principles to surgical training can foster a cooperative dynamic between teachers and residents that enhances learning outcomes. This cooperative approach is expected to benefit mentors through a sense of fulfillment in training the next generation of surgeons, accelerate skill development and strengthen professional identity for learners, and cultivate a culture of continuous improvement through ongoing evaluation and refinement of teaching/learning strategies. The integration of game theory into medical education holds broader implications beyond just surgical training. Its principles could be scaled across other medical specialties and education levels to promote more effective cooperative learning environments. Game theory concepts could also encourage interprofessional collaboration and teamwork among the broader healthcare team, leading to improved coordinated patient care. Moreover, applying these principles can serve as a model for healthcare systems policies and practices that prioritize collective good over individual interests. By incentivizing cooperation, game theory provides a framework to enhance training, teamwork, and system-level decision-making in healthcare.
Source of Funding
None.
Conflict of Interest
None.
References
- SV Kotsis, KC Chung. Application of the “see one, do one, teach one” concept in surgical training. Plast Reconstr Surg 2013. [Google Scholar]
- RK Reznick, H Macrae. Teaching surgical skills--changes in the wind. N Engl J Med 2006. [Google Scholar]
- . The Work of John Nash in Game Theory. 1994. [Google Scholar]
- R Axelrod, WD Hamilton. The Evolution of Cooperation. Science 1981. [Google Scholar]
- RJ Aumann, K Arrow, S Honkapohja. . What is game theory trying to accomplish? 1985. [Google Scholar]
- D Leedom, R Dimon. Improving team coordination: a case for behavior-based training. Mil Psych 1995. [Google Scholar]
- DW Mcfadden, M Tsai, B Kadry, WW Souba. Game theory: applications for surgeons and the operating room environment. Surgery 2012. [Google Scholar]
- AP Marco. Game theory in the operating room environment. Am Surg 2001. [Google Scholar]
- A Blake, BT Carroll. Game theory and strategy in medical training. Med Educ 2016. [Google Scholar]
- B Zheng, LL Swanström, A Meneghetti, ON Panton, AK Qayumi. Quantifying surgeon's contribution to team effectiveness on a mixed team with a junior surgeon. Surgery 2011. [Google Scholar]
- J Bernstein. Topics in medical economics: lessons of the prisoner’s dilemma. J Bone Joint Surg Am 2000. [Google Scholar]
- C Tarrant, M Dixon-Woods, A Colman, T Stokes. Continuity and trust in primary care: a qualitative study informed by game theory. Ann Fam Med 2010. [Google Scholar]
- D Itchhaporia. Game Theory, Health Care, and Economics. J Am Coll Cardiol 2022. [Google Scholar]
- B Djulbegovic, I Hozo, JP Ioannidis. Modern health care as a game theory problem. Eur J Clin Invest 2015. [Google Scholar]
- JP Sturmberg. Rebuilding trust--the real challenge for health system improvement. Eur J Clin Invest 2015. [Google Scholar]
- Introduction
- Overview of game theory, prisoner’s dilemma and the iterated prisoner's dilemma
- Summary of Axelrod's findings and principles
- The conceptual framework
- Cooperation and defection scenarios in surgical training
- Discussion
- Application of Axelrod's principles
- Assumptions and noises
- Assumptions for the system to work
- Possible Noises in the Training Environment
- Implications for surgical training
- Future Directions
- Conclusion
- Source of Funding
- Conflict of Interest